Commonly Believed Myths About Bipolar Disorder

Most people have heard of either bipolar disorder or manic depression. Unfortunately, a lot of what people believe they know about the disorder isn’t correct. Often this is due to hearing inaccurate information from others. It may also be the result of the sensationalized and faulty presentation of extreme behaviors portrayed in books on TV and in movies. But it’s important to learn the facts.
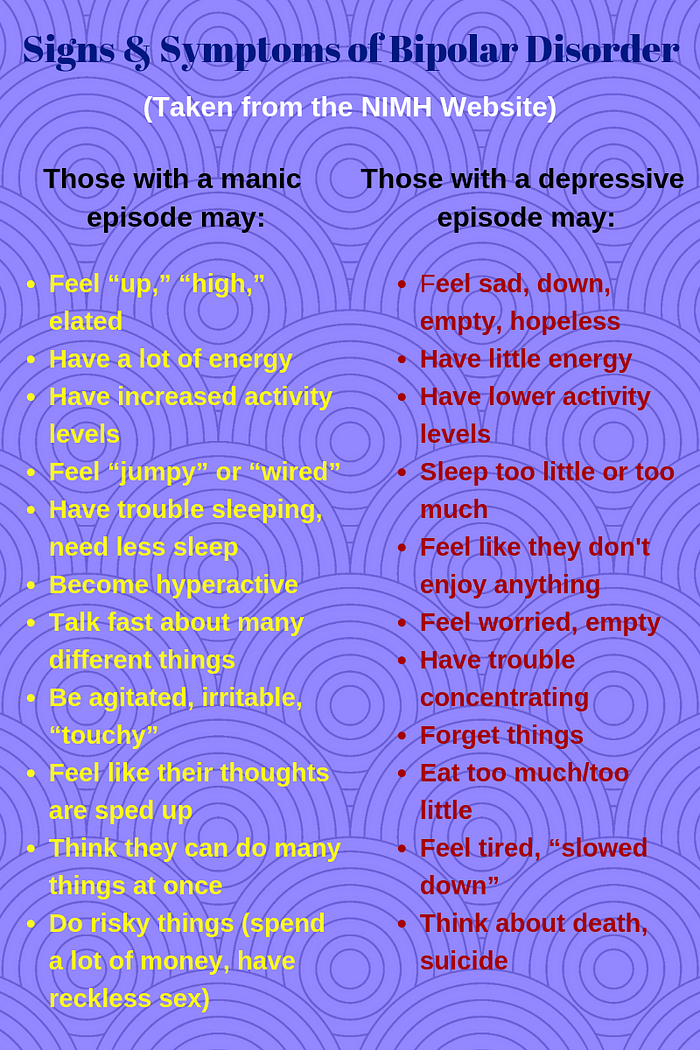
Bipolar disorder, also known as manic-depression, is a disorder of the brain that causes unusual shifts in mood, energy, and the ability to carry out day-to-day tasks. People with bipolar disorder experience episodes of unusually strong emotion, alterations in sleep patterns, abnormal activity levels, and unusual behaviors. Mood symptoms are different from the what is “normal” for the person.

Misconceptions About Bipolar Disorder
It is unlikely that everything you’ve heard about bipolar disorder is true. Learn the accurate information about the disorder so you can better understand it.
Myth: Bipolar disorder isn’t a real illness.
Truth: Bipolar disorder is cyclical brain disorder with strong genetic predispositions. A family history of bipolar disorder is the strongest risk factor for development of the illness. Most psychiatrists and mental health professionals believe that bipolar disorder is a chronic illness which similar to physical diseases requires patients to be hospitalized and need ongoing treatment. The research supports the claim that the disorder is a physiologically based illness (e.g. Charney, Ruderfer, Stahl, Moran, Chambert, Belliveau, & Bromet, 2017).
Myth: Bipolar disorder is extremely rare.
Truth: According to the National Institutes of Health, bipolar disorder affects over 5.7 million adults in the U.S. alone. This corresponds to about 2.6 percent of those over 18 years old. It’s been estimated that as many as many as 4.4% of U.S. adults will experience bipolar disorder at some time in their lives. This number is believed to be an underestimate as the disorder continues to be misdiagnosed. It is common for women, who are more likely to present in a depressed state to be misdiagnosed with unipolar depression and for men who are more likely to present in a manic state to be misdiagnosed with schizophrenia.
Myth: The diagnosis of bipolar disorder is just an excuse that people use to not have to assume responsibility for moodiness or mood swings.
Truth: The highs and lows of bipolar disorder are extremely different from common mood swings. People with bipolar disorder experience extreme changes in mood which is accompanied by changes in energy level, thought processes, interactions, motivation and the ability to function normally. They likely still have mood swings that are more normal and similar to those that individual’s without bipolar disorder have. But these don’t completely interrupt their life the way mood episode which are symptomatic of their disorder do.
Myth: Bipolar disorder can only be treated with drugs.
Truth: While medication is the recommended first-line therapy for bipolar disorder medication adherence is typically poor which leads to high relapse rates and only rare cases of full remission without additional intervention. Psychosocial therapies have also been shown to be effective as adjunctive treatments to medications.
In particular, psychoeducation and cognitive behavioral therapy have been demonstrated as effective ways to decrease relapse rates and reduce acute symptoms of depression and mania. Psychological therapy has both direct effects on symptoms and indirect effects through improved medication adherence identification of early warning signs and self-management. Family psychosocial therapy also helps reduce relapse rates by increasing awareness and support, decreasing stress and negativity and improving family communication.
Myth: Bipolar disorder is the same thing as Schizophrenia.
Truth: Bipolar disorder and Schizophrenia are two different disorders. Genetic analysis of schizophrenia and bipolar disorder is revealing a wide variety of significant contributions some of which overlap. There are both common and rare genetic variants that have been found to influence the development of each disorder again with some overlap. Other biological pathways that might contribute to both disorders include calcium channel signaling and synaptic function (e.g. Neale, & Sklar, 2015).
Additionally, in some cases of bipolar disorder, psychotic features develop. This has contributed to some of the misdiagnoses. However, it is still clear that while there may be certain areas of overlap between the two disorders, they are in fact distinct disorders.
Myth: People with bipolar disorder spend their entire life swinging from depression to mania and back again.
Truth: Mood episodes of bipolar disorder are normally relatively infrequent. The reason the disorder is so devastating is the severe effects of each episode that can have social, academic, employment, housing and legal consequences. Typically, someone with bipolar disorder experiences one or possibly two cycles a year, with the time in between being relatively normal. A big part of the problem is that, given the difficulties and pain that the episodes cause people have a great deal of anxiety related to a recurrence.
Myth: Artists with bipolar disorder will lose their creativity if they get treated.
Truth: This assumption came from a time when lithium was the only treatment for the disorder and it having sedating and slowing effects which limits arousal and activity levels. Some artists with bipolar disorder treated with lithium felt they no longer had the energy, spontaneity or creative drive to continue their artistic endeavors. Today however, there are a number of different medications and combinations of medications that don’t have the same side effects as lithium. These medication often allow artists to think more clearly an effect many have said has improved their work.
Myth: Bipolar disorder only occurs in adults.
Truth: While it is less common in children and adolescents, bipolar disorder does occur in these age groups. The lower numbers seen in youth can also be attributed in part to them not being able to engage in some of the behaviors that define symptoms such as driving too fast, excessive spending, impulsive sex and other adult behaviors.
According to NIMH, 2.9 percent of 13–18 year olds have bipolar disorder. Of children under the age of 18 almost one-third of those in the study were younger than 12, while the average age of onset was 8 1/2 years old. Bipolar disorder remains an under-recognized illness in children.
Myth: There’s only one type of bipolar disorder.
Truth: There are three main categories of bipolar disorder. Bipolar I involves full blown manic episodes. Bipolar II involves hypomanic episodes which aren’t are severe. Cyclothymic disorder involves hypomanic symptoms that don’t meet criteria for a full hypomanic episode and depressive symptoms that don’t meet criteria for a full depressive episode. Though milder the symptoms are longer lasting than what is found in bipolar I and bipolar II.
In addition to these three types, there is bipolar disorder related to substance and medication use and bipolar disorder related to another medical condition. There is also a category for those with bipolar symptoms that don’t fit with any of the defined types.
{kind=link}
0 comments